CONTINUING PROFESSIONAL DEVELOPMENT FOR NURSES
FREE! Stop That Clot: Haemostasis and anticoagulants
2 hours
2 hours
Heparin
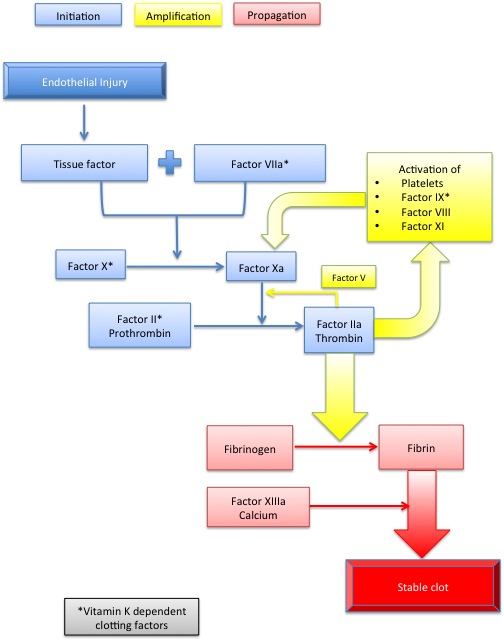
Heparin acts by binding antithrombin (AT) which allows the AT molecule to bind more readily to its target factors, in particular thrombin and factor Xa (Figure 3). Inhibition of thrombin occurs when heparin binds both AT and thrombin in a complex that prevents activation of fibrin. However once thrombin is in a clot, heparin is unable to access its binding site and is ineffective (Wong & White, 2007). Inhibition of thrombin requires a large heparin molecule because it involves binding of three molecules together. For factor Xa inhibition heparin binds only to AT and Xa. Low molecular weight heparins (LMWH e.g. enoxaparin), being smaller, are able to inhibit Xa but have a limited effect on thrombin (Gray et al., 2008). Fondaparanux is a synthetic LMWH that inhibits factor Xa exclusively.Figure 3: Coagulation
Unfractionated heparin (UFH) has a short half-life. This makes intravenous dose titration simpler but means more frequent subcutaneous dosing. Absorption after subcutaneous injection is highly variable so responses to the drug cannot readily be predicted. Testing of aPTT is required for patients on high dose UFH (Table 3).
The main advantages of LMWH are longer half-life, so less frequent dosing, and a more predictable therapeutic response so monitoring is not usually necessary (Rang et al., 2012). LMWH have fewer adverse effects than UFH, including reduced incidence of heparin-induced thrombocytopenia (HIT). HIT is an immune reaction triggered by heparin binding to platelets. It may develop 2 to 14 days after commencing heparin therapy and causes platelet destruction, injury to blood vessels, thrombosis and disseminated intravascular coagulation (Rang et al., 2012). There is no difference in haemorrhage rates between UFH and LMWH (Gray et al., 2008) but the heparin antagonist, protamine, is less effective with LMWH.
Unfractionated heparin (UFH) has a short half-life. This makes intravenous dose titration simpler but means more frequent subcutaneous dosing. Absorption after subcutaneous injection is highly variable so responses to the drug cannot readily be predicted. Testing of aPTT is required for patients on high dose UFH (Table 3).
The main advantages of LMWH are longer half-life, so less frequent dosing, and a more predictable therapeutic response so monitoring is not usually necessary (Rang et al., 2012). LMWH have fewer adverse effects than UFH, including reduced incidence of heparin-induced thrombocytopenia (HIT). HIT is an immune reaction triggered by heparin binding to platelets. It may develop 2 to 14 days after commencing heparin therapy and causes platelet destruction, injury to blood vessels, thrombosis and disseminated intravascular coagulation (Rang et al., 2012). There is no difference in haemorrhage rates between UFH and LMWH (Gray et al., 2008) but the heparin antagonist, protamine, is less effective with LMWH.